
A thankful heart is the parent of all virtues. This thanksgiving may you give thanks for everything you are blesses with this happy occasion and wish you lots of happiness!
A thankful heart is the parent of all virtues. This thanksgiving may you give thanks for everything you are blesses with this happy occasion and wish you lots of happiness!
Lupine Publishers | Scholarly Journal Of Psychology And Behavioral Sciences

Introduction
The interlocked
relationship between mind and body has increasingly resulted in modern medical
practices’ use of biopsycho- social and patient-centered models that emphasize
various psychological and environmental factors [1-3]. In particular,
patientcentered approaches are characterized by a serious consideration of
patients’ views, preferences, values, and economic resources [4]. In addition
to positively affecting various medical outcomes and patient satisfaction
levels, patient-centered approaches have been shown to reduce the use of
healthcare services, diagnostic tests, prescription, referral, and
hospitalization, along with total annual healthcare expenses [5,6]. Given that
visiting a physician may in itself induce considerable worry and anxiety in patients
[7], physicians’ interpersonal communication competencies and styles can
directly influence patients’ self-expression by providing them with a sense of
being listened to and understood, which in turn acts on several factors such as
patients’ anxieties about their illness, hope for a cure, and adherence to the
treatment [8]. In the treatment of somatic diseases, talking about disease
perception reveals the therapeutic effect of talking [9]. In this regard,
empathy refers to a “cognitive quality” that by its interpersonal nature
involves a physician’s capacity to understand and communicate about patients’
experiences, anxieties, and viewpoints [10,11]. Empathy has been reported to
reduce patients’ anxiety and stress levels and to considerably influence positive
health outcomes [12]. More specifically, physicians’ empathy has been shown to
be significantly associated with diabetes patients’ clinical outcomes and
result in shorter periods of the common cold [13-16].
As these studies point
to a concrete and measurable effect in the immune system induced by a
positively experienced subjective feeling, they further substantiate the strong
relationship between mind and body. Among the factors that have transformed the
physician-patient relationship from Emanuel’s paternalistic model to a
conciliatory model are the rising socioeconomic level with social development,
medical technologies that improve the quality of life, the development of
patients’ rights, patients’ greater knowledge of their rights, developments in
the concept of seeking rights, physicians and patients putting more value on
human rights, the widespread implementation of legal responsibilities and
sanctions on physicians and patients, legal obligations, the application and
dissemination of the understanding of quality in healthcare, rising health
literacy, and the existence of complaint mechanisms through communication
centers of public institutions [17]. Studies supporting patients’ empathy
expectations in Turkey [18-23] as well as focusing on patient-physician
communication show that empathy stands out as a very important element,
sometimes alone and sometimes together with other variables [24-26].
There are many studies
that evaluate empathy education and empathetic attitudes of students in the basic
medical education process in medical schools and investigate how empathy can be
developed [27-33]. As another significant variable of this study, cognitive
flexibility is regarded as a form of fluid intelligence marked by the skill of
providing alternative solutions to different situations [34]. This construct is
closely related to the neuro-psychological concepts of role- and
perspective-taking, which entail numerous cognitive flexibility dimensions such
as understanding others, selecting appropriate behavior, thinking about and
generating different ideas, possessing a repertoire for different responses,
and exchanging ideas with others in decision-making [35]. Literature on
cognitive flexibility related to personnel working in the healthcare field is quite
limited. A study on nurses found that coping skills and flexibility were
positively correlated with psychological adjustment [36]. A study of medical
students and residents showed that incorporating cognitive flexibility and
perspective-taking skill instruction has implications for reducing conflict and
stress, as well as improving wellness levels [37]. Empirical studies
demonstrate that increased cognitive flexibility is linked to reduced levels of
experiencing social difficulties, stress, depression, anxiety, and rage
[38-42]. Conversely, cognitive flexibility has been found to be related to
positive personal outcomes such as critical thinking, selfesteem, social
skills, self-competence, and coping with stress [43- 45].
Although limited amount
of evidence exists in the literature, there are several empirical studies that
substantiate the relationship between empathy and cognitive flexibility. In one
major example, neurological patients with various etiologies and cerebral
lesions were found to manifest significantly lower empathy than healthy normal
adults. The same study found significant correlations, ranging from 0.5 to 0.6,
between cognitive flexibility and empathy scores [46]. These data support the
idea that cognitive thinking may be closely linked to empathic behavior either
via granting a precognitive skill or by being part of another common basic
process. The present study is designed to make comparisons between Turkish
practitioner and specialist physicians in terms of empathy, cognitive flexibility,
and interpersonal relations styles. In so doing, it tests the question of
whether practitioners’ long-term interactions with their enrolled patients
(i.e. spending more time with them, knowing them better) or specialists’ longer
training histories are correlated with increased empathy and cognitive
flexibility levels.
Methods
Participants
It is included family
physicians, who have completed 6 years of medical training and specialists who
have completed an additional 5 years. Family physicians see the patients
registered with them and specialists see patients who can make an appointment
anytime and anywhere. Inclusion criteria for data collection were determined as
for specialists who work as clinician. Branches of specialists: 5 orthopedics, 8
chest diseases, 1 neurology, 4 obstetrics, 3 infectious diseases, 2 internal
medicine, 1 physical therapy, 1 pediatric, 3 ENT, 2 urology. General
practitioner work as clinician. Thus, the sample of the present study comprises
60 participants, i.e. 30 practitioners and 30 specialists. Demographically, 40%
of the practitioners and 47% of the specialists were women. Additionally, 90%
of the practitioners and 97% of the specialists were married. The age average
for practitioners and specialists was 45.5 and 43.2, respectively. As mentioned
above, participants’ working posts involved family health centers and state or
training and research hospitals. Paper-and-pencil questionnaires were filled
out by volunteer participants themselves in the major cities of Istanbul and
Ankara between January and April 2019.
The questions that the
study aims to measure in terms of the variables included are as follows:
Do long-term interaction
and being familiar affect physicians’ interpersonal relationship styles?
Does residency training
affect specialist’ relationship styles?
Assessment Instruments
To address its research
questions, this research employed the Jefferson Scale of Physician Empathy, the
Cognitive Flexibility Inventor, the Interpersonal Relationship Scale, and a
sociodemographic form.
Jefferson scale of physician empathy
The Jefferson Scale of
Physician Empathy (JSPE) is a 20-item, 7-point Likert-type scale. In a sample
of medical doctors, its internal consistency was found to be around .80. In the
Turkish context, this scale was adapted by Malkondu in 2006 and its validity-reliability
study was done on a sample of dentists [47].
Cognitive flexibility inventory
Developed by Dennis and
Vander, the Cognitive Flexibility Inventory involves 20 questions and two
subscales entitled “alternatives” and “control” [28]. The alternatives subscale
comprises 13 items that tap into the extent to which an individual is able to
find alternative solutions to difficult conditions or can form alternative
explanations for life situations and people’s behaviors. The control subscale
is constituted by items that measure to what extent these predicaments can be
controlled [48]. The Cronbach’s alpha values for alternatives and control
subscale were reported as .91 and .84, respectively. Higher scores are
indicative of increased cognitive flexibility [28]. Validity and reliability
research for the scale’s Turkish version was undertaken, who found Cronbach’s
alpha values of .90 for the whole scale, .89 for the alternatives subscale, and
.85 for the control subscale.
Interpersonal relationship scale
Developed by this
31-item, 3-point Likert-type scale assesses individuals’ interaction styles
with others. Two subscales measure nurturing and restraining styles,
respectively. Nurturing relations involve skills such as expressing one’s needs
in an open manner, treating the other person with a respectful and accepting
style, and employing a constructivist discourse. Conversely, restraining
communication styles are marked by behaviors such as selfrighteousness,
condescension, short temper, verbal abuse, and mockery. The scale has been used
in many studies and evidence has been obtained that it is valid and reliable
[49-52] Subscales for nurturing styles, in turn, tap into open and respective
styles, while the restraining styles subscale further comprises egocentric and
condescending styles. The internal consistency coefficient for the whole scale
was measured as .79. Cronbach’s alpha values for open, respectful, egocentric,
and condescending styles were .73, .70, .56, and .78, respectively.
Results
As reassessed from the
data, the Cronbach’s alpha coefficient for the empathy scale turned out to be
.847, while the cognitive flexibility subscales of control and alternatives had
internal consistency values of .653 and .749, respectively. The interpersonal
relationship subscales’ alpha coefficients ranged from 0.653 to 0.749. In terms
of between-group comparisons, Mann-Whitney U tests indicated that, although
specialists’ empathy level was higher than practitioners, the difference was
not statistically significant. With respect to cognitive flexibility
comparisons, Mann-Whitney U and t-tests substantiated that only the cognitive
flexibilityalternatives subscale was significantly higher in specialists than
practitioners. The associated values for these comparisons are shown in Tables
1,2. Interpersonal relationship style comparisons centered on nurturing
(open-respectful) and restraining (ego centric-condescending) styles. As scores
for open and egocentric styles were normally distributed for both groups,
t-tests were employed for comparisons. Conversely, distributions for respectful
and condescending styles were not normally distributed. Thus, the Mann-Whitney
U test was preferred for comparisons in these domains. Accordingly, results
indicated that specialists received significantly higher scores than
practitioners in nurturing styles and significantly lower scores in restraining
styles [Table 3].
Table 1: Comparison
of empathy levels between specialists and practitioners.

According to the
Mann-Whitney U test, although specialists’ empathy levels were higher than
practitioners’, this difference was not statistically significant, (p>0.05).
Table 2: Comparison
of cognitive flexibility levels between specialists and practitioners.

*p<0.05
According to the
Mann-Whitney U and t-tests, alternatives subscale was the only statistically
significant difference, and scores were higher for specialists, (p<0.05).
Table 3: Comparison
of interpersonal relationship styles between practitioners and specialists.

*p<0.05
According to
Mann-Whitney U and t-tests, significant differences were found in terms of
open, respectful, and condescending styles between practitioners and
specialists. Specifically, specialists displayed higher open and respectful
style scores and lower condescending style scores.
Spearman-Brown
correlational analyses revealed a significant positive association between
empathy and cognitive flexibility for practitioners. Similarly, for this group,
the relationship between empathy and respectful relationship styles was also
significantly positive, while the correlation between empathy and condescending
styles was significantly negative [Table 4]. Specialists’ correlations between
empathy and cognitive flexibility and relationship styles were not significant
[Table 5]. Regarding correlations between cognitive flexibility and
relationship styles, for practitioners, control and alternatives subscales were
moderately associated with respectful styles. For specialists, cognitive and
alternatives subscales were significantly related to open styles. For this
group, an alternatives subscale was also moderately related to respectful
styles. These significant positive associations are shown in Tables 6 and 7,
respectively. Gender and marital status were not significantly related to
specialists’ or practitioners’ empathy tendencies, relationship styles,
cognitive flexibility total, or subscale scores. For practitioners, having
longer careers contributed significantly to increased empathy, cognitive
flexibility levels, and nurturing styles. For this group, age and cognitive
flexibility was also positively related. For specialists, age and working
duration were not significantly correlated with empathy levels, relationship
styles, or cognitive flexibility levels. These results are shown in Table 8. According
to the Spearman-Brown analysis, significant moderate associations were found
between cognitive flexibility alternatives and respectful and condescending
styles that were positive and negative in nature, respectively. There was also
a positive moderate correlation between cognitive flexibility control and
respectful style.
Table 4: Correlations
between empathy and cognitive flexibility and empathy and interpersonal
relationship styles in practitioners.

*p<0.05
According to the
Spearman-Brown analysis, positive significant correlations were found between
empathy and cognitive flexibility control and alternatives subscales. Empathy
was also positively related to respectful styles. The sizes of these relations
were moderate. Another moderate correlation was found between empathy and
condescending styles that was negative in nature.
Table 5: Correlations
between empathy and cognitive flexibility and empathy and interpersonal
relationship styles in specialists.

Table 6: Correlation
between cognitive flexibility and interpersonal relationship style in
practitioners.

*p<0.05
According to the
Spearman-Brown analysis, significant moderate associations were found between
cognitive flexibility alternatives and respectful and condescending styles that
were positive and negative in nature, respectively. There was also a positive
moderate correlation between cognitive flexibility control and respectful
style.
Table 7: Correlation
between cognitive flexibility and interpersonal relationship style in
specialists.

*p<0.05
According to
Spearman-Brown correlation, the cognitive flexibility alternatives subscale was
positively and moderately related to open and respectful styles. The cognitive
flexibility-control subscale was positively correlated to open style.
Table 8: Associations
between Empathy/Cognitive Flexibility and Age/Working Duration.

*p<0.05s
Discussion and Conclusion
Discussion
Findings revealed
specialists’ empathy and cognitive flexibility scores were generally higher
than practitioners’, yet the only statistically significant dimension was
cognitive flexibilityalternatives in specialists.
In interpersonal
relations, significant differences in terms of open, respectful, and
condescending communication styles demonstrated that, compared to
practitioners, specialist physicians were again more competent in these areas.
These findings do not corroborate our tentative assumption when undertaking the
study, namely that due to familiarity and longer interactions with their
patients, practitioners should exhibit higher empathy, cognitive flexibility,
and communication competence. Our particular pattern may have stemmed from
various factors: First, with respect to cognitive flexibility, due to certain
preexisting cognitive skills, individuals who become specialists may be
predisposed to more competently assess alternatives in particular situations
and problems. Indeed, [53] proposed that the predominant characteristic of
experts is the ability to manipulate versatile mental representations, which in
turn enables them to adapt better to environmental changes and use their
knowledge more efficiently among different tasks. Alternatively, one may
consider the effect of specialists’ education in terms of both different
cognitive skills acquired and being exposed to courses on patient-doctor
interactions. It is conceivable that different specialist branches, the
cultures of hospitals and medical schools, socioeconomic status, or even cities
of residence may play a role in augmenting or hindering cognitive flexibility,
empathy, and interpersonal relationship style. In this regard, future studies
may include these variables to determine both their unique and interactive
effects for various professionals in the medical field.
Although not displaying
a statistically significant difference, higher empathy levels and interpersonal
relations competence of specialists may be linked to particular predicaments of
the medical system in Turkey. In Turkey, practitioners regularly receive a
burdensome number of registered patients. In this sense, it is reasonable to
suggest that practitioners may have developed certain emotive strategies to
mitigate the emotional burden that accompanies personal interactions with their
patients. Alternatively, the mundane and repetitive tasks of referrals to
specialists and renewing prescriptions may also hamper the tendency to develop
a genuinely empathetic understanding of patients’ problems and emotional
states. Conversely, specialists in Turkey accept additional patients in return
for extra income, which offers them an opportunity to control the overburden
they experience. These points highlight the importance of considering the
significant role that the nature of healthcare systems may play in determining
the quality of interpersonal communication and empathetic interaction. It is
particularly telling that both specialist and practitioner empathy scores in
Turkey are well below those reported by international studies, which lends
support to the idea that predicaments in healthcare systems may greatly
compromise cognitive flexibility and empathy. As compared to our scores of
101.30 for specialists and 97.63 for practitioners. Reported international
physicians’ empathy levels in human-centered and technology-centered specialty
fields as 112.9 and 106.9, respectively. Average physician empathy levels were
found to be 120 in the United States [54-60].
In another major
finding, in a practitioner sample within group analyses, the present study
substantiated empathy’s significant relation to cognitive flexibility and
interpersonal relations. These findings resonate with a prior study on Turkish
university students [52] in which, as in this study too, empathy was found to
be positively associated with open and respectful styles and negatively linked
to condescending styles. Since in our study, empathy in specialists was not
correlated to cognitive flexibility or communication style, one may consider
the idea that, for specialists, the more intermittent and impersonal nature of
doctor-patient interactions in the Turkish healthcare system enables the
acquisition of satisfactory communication skills mainly via cognitive skills.
Conversely, for health professionals such as practitioners and nurses who
interact more closely with patients, communication skills may be induced mainly
along the path of empathy.
Notwithstanding fields
or branches among health professionals, the present study can be considered a
noteworthy contribution to international research that investigates questions
regarding empathy, cognitive skills, communication, and patient outcomes for
healthcare professionals and workers at large. Indeed, a recent upsurge in
international studies started to increasingly point to relations of these
kinds. To give a few examples, prior research found a positive relationship
between empathy and interpersonal relations in nursing students [61,62] and
similarly posited positive relationships among empathy, perspective-taking,
nurturing care, and friendly-harmonious relationship types in medical students
[63]. Recently a strong relationship was suggested between empathic thinking
and perspective-taking [64]. Hence, the present study lends support to the idea
that the empathic and communicational skills of medical professionals should be
one of the major avenues of research for promoting patient outcomes [65- 67].
This study offers ideas
as to why training intervention is needed to improve communication and
interpersonal relationships, and also includes suggestions about what the
training program should cover. Some limitations should also be noted. The
rather small sample sizes, including 30 participants for each group, and
nonrandom, voluntary sampling procedures in this study should be considered
caveats preventing satisfactory representativeness and generalizations around
the globe. Additionally, variables such as doctors’ and patients’ personality
traits and cultural and socioeconomic backgrounds were excluded from analyses.
Lastly, our measuring instruments relied on self-report scales and are thus
subject to biases rooted in the conveyance of subjective experience. These
points should be taken into account by researchers while drawing cautious inferences
for future research studies.
Conclusion
All in all, this study
provides support to bio-psycho-social model patient-centered approaches and
suggests their adoption positively influences patients’ psychological, mental,
and physical health. Hence, the cultivation of an understanding recognizing the
importance of interpersonal relations, communication skills, and interaction
between the mind and body seems to be a worthwhile endeavor in the medical
field. The long-term articulation of costeffective methods in healthcare
systems – primarily training in factors promoting interpersonal relationships
such as empathy and cognitive flexibility – would positively contribute to more
efficient processes of diagnosis and therapy based on fulfilling interactions between
physicians and patients.
https://lupine-publishers-psychology-journal.blogspot.com//
Lupine Publishers | Scholarly Journal Of Psychology And Behavioral Sciences

Abstract
The generalisation of
responses to different stimuli depends on the ability to create associations
between stimuli. Stimulus generalisation can be performed for different stimuli
or for different contexts in which the same stimulus is perceived. This study
investigated the stimulus-generalisation abilities of horses in different
contexts. Sixteen horses were involved in this study. During the learning
activity (LA), horses were given the chance to choose between two geometrical
figures (a triangle and a circle) to obtain a food reward; the circle always
corresponded to the correct choice. The rule was considered learned if a horse
was correct more than 70% of the time and made 4 consecutive correct choices.
Then, a generalisation test (GT) with ten devices (5 circles, 5 triangles) was
created to test generalisation. Only eleven horses respected the learning
criteria and were included in the generalisation test. A significant difference
in the number of correct choices between the learning activity and the generalisation
test was observed (Wilcoxon signed-rank test, S=-33; p=0.001; LA: median=6,
min=3, max=9; GT: median=3, min=0, max=5). There was no significant difference
in the number of incorrect choices between the two tests (Student’s t test,
t=-0.91; DF=10; p=0.384). A significant difference in the total number of
choices between the two tests was observed (Student’s t test, t=2.56; DF=10;
p<0.05). This experiment suggested limits in the capacity of horses to
generalise a well-known task in different contexts. Because horses are often
exposed to different environments or contexts, these results provide
interesting and applicable knowledge for equine training and management.
Keywords: Behaviour;
Equine Management; Generalisation; Horse; Learning; Welfare
Introduction
Horses are involved in
many activities that have evolved over time and have changed the human-horse
relationship [1]. Currently, horses perform sports and work activities that
require adaptation to different contexts [2,3]. Horses are continuously
challenged from physical and psychological perspectives and need to understand
information provided by different persons or in different contexts [3,4]. To
succeed in equitation, horses must learn different categories of exercises that
are demanded by riders [5]. However, rider weight and posture, as well as the
intensity applied to cues, are variable, which often results in differences in
the information perceived by the horse [6]. Nevertheless, horses have an
incredible behavioural flexibility that allows them to adapt their responses to
the intensities of the cues given by different riders [7-10]. In addition,
horses are athletes that often participate in competitions. Competition has
been shown to induce physiological modifications in horses related to stress
[5-11]. In competition, riders expect their horses to ignore external stimuli
and to perform as usual in response to trained cues, which requires horses to
generalise those cues from a training environment to a new context with
multiple stimuli, such as the presence of the public [11]. The same situation
might happen each time horses experience a change of ownership or a change in
their living conditions [12]. To summarise, equine living conditions, training
and competitions are full of different stimuli that challenge horses’ coping
strategies [13-15]. In this context, it is important to understand that the
generalisation of a stimulus implies that animals can form associations between
different stimuli (Nicol, 2005). Horses are requested to generalise their
responses to different stimuli over training, either through positive or
negative reinforcement [7]. Stimulus generalisation could be performed from a
group of stimuli with some similarities (e.g.: curved shapes) to a novel
stimulus, which share the same similarities (e.g.: a circle) [16]. However,
stimulus generalisation may also occur as the generalisation of a defined
stimulus to different contexts [17]. Stimulus generalisation to new contexts
appears to be difficult for horses [18-20].
Hence, the
generalisation of a well-known stimulus to different stimuli is a factor in
equine management and welfare [5]. This means that providing more efficient and
reliable training methods for riders and owners can increase the welfare of
horses [6,11]. Therefore, to efficiently improve horse welfare in equine
husbandry and training, riders and owners should learn from scientific
knowledge instead of following common beliefs [15]. The present study aimed to
investigate the ability of equines to generalise a learned task, based on the
same rule, to different contexts. We hypothesised that horses would show the
generalisation of a learned stimulus to a novel test in a different setting.
Methods
Subjects
Sixteen horses (11
geldings; 5 females) older than eighteen months (11.5 ± 6.14 years) were
involved in this study. All horses participated in equestrian activities on a
daily basis. A visual examination was performed by a veterinary doctor to
ensure that none of the animals had vision issues that could impair the tests.
This study was divided into two learning events. All animals were submitted to
a learning activity (LA), which was a reproduction of the test used. The LA
intended to show the discriminative rule to the horses, enabling the selection
of a population of horses that understood the rule before performing the second
test. The discriminative rule was considered learned if a horse was correct
more than 70% of the time and made 4 consecutive correct choices. Only horses
that respected these criteria were included in the second test, which was a
generalisation test (GT).
Material
“Philbox”, the
dispositive adapted and he was used for the LA in this experiment (Figure 1).
The device consisted of two white panels; removable black shapes (a circle or a
triangle) could be placed in front of the panels, and a hidden operator could
insert treats on a food tray through a hole under each shape. A second operator
led the horses to the panels. Ten “Pesadelo” devices were created to test the
equine generalisation abilities (Figure 2). Each of these devices included a
tilting mechanism, with one black shape painted on a white panel on the top (5
had a circle, and 5 had a triangle) and an inverted container on the bottom.
Treats were placed in the containers, which each had a cover. For all devices
marked by a circle, this cover was pierced such that the treats fell on the
ground when the animals pushed or pulled the panel. For devices marked by a
triangle, the cover was intact, so the treats did not fall when the animal
pushed or pulled the panel. Some holes were created on the container to ensure
that both devices had the same odour, regardless of cover type. There was a
tray under each container. No operators were needed to run this device.
Figure 1: Philbox. The Philbox is a modified device for performing cognitive
tests. The Philbox includes two removable geometrical shapes (circle and
triangle) and a hidden operator who provides treats when the animals touch the
panel with the correct shape.

Figure 2: Pesadelo. A Pesadelo is a device created to perform cognitive
tests. The device includes a tilting mechanism with a shape-marked panel on one
side and a treat in a container on the other side. To obtain the treat, a horse
must push the panel (circle or triangle), such that the shape-marked panel
tilts down and forward, the container tilts up and backward, and the treat
drops onto the floor.

Procedure
A habituation session to
the Philbox device was performed, as described. The setting was presented to
the subjects, and spontaneous approaches and interactions with the device were
rewarded with a treat. The session consisted of twelve efforts with the shapes
removed from the devices. The initial phase of the session included 6 attempts
(3 on the right and 3 on the left) using a treat on the panels as a lure; an
additional reward was given each time the horses touched the panels. The horses
then made 6 more attempts, for which they received a reward only upon touching
the panels. A habituation session for the Pesadelo device was also performed to
show horses the mechanism of pushing/pulling the panel to obtain treats. For
this session, two devices with the shape panel replaced by a whole white panel
were used. Horses were given 3 minutes of free contact with the two devices, in
which any spontaneous contact with the panel was reinforced with a treat that
felt from the container. For this purpose, each time a horse obtained a treat,
an operator led the horse to the other device, while a second operator refilled
the empty container with treats.
The LA were performed
using the Philbox device and lasted five minutes for each horse. Horses had the
possibility to choose between the shapes and received a reward (food treat)
upon touching the correct shape (always the circle) with their noses (positive
reinforcement). The development of a side preference was avoided by following
predefined sequences of four figures, with a randomised order of appearance,
thus avoiding any recognisable pattern. In addition, a food treat was hidden
behind each shape to provide the same olfactory cue for both the circle and
triangle. There was no limit to the number of attempts horses could perform
during the 5 minutes of the test. Once a choice was made, horses were walked
around by the operator and returned to the starting position. Thus, the horses
that made choices faster could perform more attempts during the 5 minutes of
the test. Each horse was led to a distance of 1.5 metres in front of the panels
and then freed to interact with the setting. The operator stopped at 1.5
metres, stayed in a neutral position, and did not interact with the animal
until a choice was made. Horses that made 70% or more correct choices, with at
least 4 consecutive correct choices, were subsequently included in the GT.
There was a time lapse of 48 hours between the two tests for all horses. The GT
lasted 5 minutes for each horse. The setting consisted of ten Pesadelo devices
(5 circles and 5 triangles) placed in a controlled testing area inside of a
riding arena (Figure 3). Each device provided only one treat. The devices were
randomly positioned in the setting area to permit the horse to easily access
the two options (triangle and circle). Each horse was completely free in the
testing area, and the operator left the riding arena and the visual field of
the horse. The performance parameters for both tests included correct and
incorrect choices and the total number of choices. For the GT, a choice was
considered correct both the first and second time a horse pushed/pulled the
same panel with a circle, even if the treat reward was only achieved during the
first interaction. The same rule was applied for incorrect choices. If the
horse returned to the same device a third time, that choice was not considered,
neither correct or incorrect. Each horse was considered its own control.
Figure 3: Generalisation test setting. Ten Pesadelo devices were positioned
in a controlled area to test equine generalisation capacities.

Statistical Analysis
Statistical analysis was
carried out using 9.4 SAS software (2002-2012 by SAS Institute Inc., Cary, NC,
USA). The significance threshold was classically fixed at 5%. Comparisons among
the horses’ performances during the LA and the GT involved paired samples. To
use the paired Student’s t test, normality was tested on the difference of the
results in the LA and in the GT for the following parameters: “correct
choices”, “incorrect choices” and “total number of choices”. For the “correct
choices”, assumption of normality was not verified, so the non-parametric
signed-rank Wilcoxon test was preferred. Normality was verified for “incorrect
choices” and “total number of choices”; hence, the parametric Student t test
was used.
Results
From the 16 initial horses,
five did not learn the discriminative rule, so they were not included in the
GT. The final population of horses comprised 11 subjects (7 geldings; 4
females). Only these horses were considered for the statistical analysis.
Figure 4 compares these horses’ performances between the two tests. A
significant difference in the number of correct choices between the learning
activity and the generalisation test was observed (Wilcoxon Signed-Rank test,
S=-33; p=0.001; LA: median=6, min=3, max=9; GT: median=3, min=0, max=5). Horses
made two times fewer correct choices in the GT than in the LA. There was no
significant difference in the number of incorrect choices between the two tests
(Student’s t test, t=-0.91; DF=10; p=0.384).
Figure 4: Comparison of horses’ performances in the two tests (mean ± SD of
choices). The learning activity is represented by light grey, and the
generalisation test is represented by dark grey. ***: highly significant
p-value, p=0.001; *: significant p-value, p<0.05.
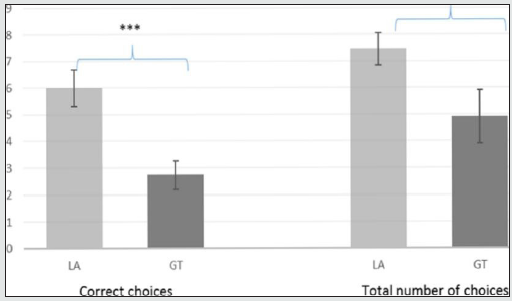
A significant difference
was observed in the total number of choices between the two tests, (Student’s t
test, t=2.56; DF=10; p<0.05). Horses made a greater number of choices in the
LA than in the GT.
Discussion and Conclusion
This experiment showed that
horses who learned a specific discrimination task had a lower performance when
the task was presented for the first time in a different context and setting.
This result was emphasised by the decrease in the total number of choices and
the number of correct choices between the learning and the GTs. The absence of
a significant difference in the incorrect choices between the tests was
probably related to the reduced total number of choices in the GT when compared
to the LA. Horses made fewer attempts in the GT and often chose the wrong shape
or device. The decrease in the horses’ performance between tests suggests that
the generalisation of a learned task between contexts might require training
and repetition. Even if the discriminative rule had been the same in both
tests, the setting was completely different. The GT involved a
three-dimensional setting with multiple devices, with only one positive
reinforcement per device. For the LA, horses had panels simultaneously
presenting all possible choices in their visual field, while for the GT, it was
essential for horses to walk between the devices to reach all of them. The new
context of the test can have impacted the performance in the GT. In addition,
for the LA, an operator was always present. His presence could have represented
a help for the animal. However, in our study, the operators were trained to
stay in a neutral position and avoid any interaction with the horses to prevent
them from influencing the horses’ choices. One could argue that the time (i.e.
48h) between tests could have a role in memorisation and, consequently, the
generalisation of the rule. Nevertheless, memory in horses seems to be reliable
and longlasting through life, as described by Hanggi and Ingersoll (2009).
Our results differ from
those of Christensen et al. (2008), who conducted a study in which horses were
submitted to a GT between stationary objects of the same colour with varying
shapes in the same setting conditions. That study changed the rewarded shape
between tests, while in the present study, the rewarded shape (the circle)
remained the same between tests, but the setting was changed. Therefore, the
generalisation of a well-known stimulus might depend on the context and
environment [20]. This hypothesis is supported by the results, who created a
setting with a lever near two buckets in an area open to horses. Horses learned
that once they pressed the lever, they could have a food reward. Then, in a
Y-maze test, a lever pointed to the direction of the correct side of the maze,
where horses could find a food reward. They found that horses’ performance
decreased from the bucket test to the Y-maze test. Even if the rule, i.e. the
presence of a lever, was the same to obtain a food reward in both tests, the
manner to follow the rule was different. Indeed, horses are accustomed to
exploring new objects by touching or licking them; therefore, the exploratory
behaviour of horses may have spontaneously provided the manners to use the
lever to get a reward. However, in the Y-maze, this natural behaviour does not
lead to any reward, so horses probably needed to find new coping strategies,
which requires time and experience. Conversely, in our study, horses could
obtain the reward by following the same rule with the same manner in the two tests,
i.e. by pressing on a circle, which provided the same reliable information that
horses could use for both tests. We observed a decrease in horses’ performances
between the two tests, indicating that context features other than the manner
to follow the rule can influence the generalisation abilities of horses.
Research findings are of
great importance and should be considered in equine welfare and management
because these findings often contradict commonly held beliefs about equine
cognition and learning abilities [10-16]. Horses are part of a worldwide market
and are moved across countries, which often implies regrouping with other
conspecifics [18].
The ease of habituation
to new living conditions is a serious welfare concern in horses that often results
in misunderstandings in the human-horse relationship [4,6]. For example, if a
horse is moved to novel husbandry conditions, its behavioural response to a
well-known stimulus and the resulting coping strategies could be different from
the original response and strategies, and these differences could be justified
by the context modification, regardless of the horse’s previous habituation to
that stimulus. The same problem could occur during competition because horses
must perform previously learned exercises in new contexts [5]. In conclusion,
this experiment suggested some limits in the capacity of horses to generalise a
well-known task to different contexts. This study demonstrated that horses’
perception of different stimuli is context specific. Increasing our knowledge
about the generalisation abilities of these animals is of great importance to
improve equine management and training. Further research is still needed to
fully understand horses’ generalisation abilities, especially focusing on the
ability to generalise similar information in the same context, and to measure
the influence of this ability on equine management and training.
https://lupinepublishers.com/psychology-behavioral-science-journal/pdf/SJPBS.MS.ID.000214.pdf
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Psychology And Behavioral Sciences Please Click
Here: https://lupinepublishers.com/psychology-behavioral-science-journal/
To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online

