Wednesday, 27 November 2019
Lupine Publishers: Lupine Publishers | Selected Methods of Spatial An...
Lupine Publishers: Lupine Publishers | Selected Methods of Spatial An...: Lupine Publishers- Environmental and Soil Science Journal Spatial analysis in GIS Wednesday is based on complex techniques, the r...
Lupine Publishers | Psychiatric and Medical Comorbiditiesinpatients With Bipolar Disorder: A Hospital Based Study
Lupine Publishers | Scholarly Journal Of Psychology And Behavioral Sciences

Abstract
The two most common bipolar disorders are
bipolar I disorder and bipolar II disorder. Comorbid psychiatric disorders
usually precede the onset of bipolar disorder. Bipolar disorder often coexists
with other Axis I and Axis II disorders. Studies have shown that patients with
mood disorders have more comorbid medical illnesses. Research has suggested
that that there may be underlying biological mechanisms linking mood disorder
and many medical illnesses.The current study will determine the psychiatric and
medical disorders in a sample of patients with bipolar affective disorder in a
general hospital setting.
Aims and Objectivest: study the
socio-demographic profile of patients with Bipolar affective disorder, to study
the prevalence of psychiatric comorbidities in patients with Bipolar affective
disorder and to study the prevalence of medical comorbidities in patients with
Bipolar affective disorder.
Methodology: This
cross-sectional study was conducted at the department of Psychiatry,
Sher-I-Kashmir Institute of Medical Sciences (SKIMS), Medical College and
hospital, Bemina, Srinagar, Jammu and Kashmir. Psychiatry department at
SKIMS-MC is a General Hospital Psychiatry unit.
Results: In the present
study the mean age of patients was 34.3 years, Majority of patients were
females, married. In this study, obesity/ weight gain (n=52), chronic headache
(n=45), hypertension (n=30), elevated serum lipids (n=28), thyroid disorders
(n=19), diabetes (n=12), GERD (n=9), CAD (n=4), epilepsy (n=2), COPD (n=2),
bronchial Asthma (n=1), Parkinson’s disease (n=1), CKD (n=1) were among the
medical comorbidities. In this study the most prevalent psychiatric disorders
in patients with BPAD were Substance use disorder (n=32), somatoform disorders
(n=18), Generalized anxiety disorder (n=12), obsessive and compulsive disorder
(n=11), panic disorder (n=9), simple phobia (n=7), eating disorders (n=5),
social phobia (n=4), and PTSD (n=2).
Conclusion: The current study
suggested that patient suffering from bipolar affective disorder are at increased
risk of developing medical or psychiatric comorbidities. It is very important
for the treating physician to be aware of the prevalent medical and psychiatric
conditions patients with bipolar affective disorders and knowledge of these
comorbidities help in prevention, early detection and treatment of such
illnesses as well will improve treatment response and prognosis in bipolar
patients itself. Awareness among healthcare professionals about the risks to
which patients withaffective disorders are exposed is of great importance, as
the medical illnessesare likely to coexist with a mood disorder, which may help
to improvediagnostics and management and therefore clinical and social care for
patients. Overall, the presence of comorbidities in BPD has negative prognostic
implications for psychological health and for medical well-being and longevity.
In order to improve quality of life, prognosis and life expectancy for those
with these illnesses, it is important that further researches on this topic should
be continued.
Keywords: Bipolar Disorder; Psychiatric
Comorbidity; Medical Comorbidity; Anxiety Disorders; Substance Abuse
Background
A complex, chronic mood disorder
involving repeated episodes of depression and mania/hypomania is referred as
Bipolar disorder [1]. The two most common bipolar disorders are bipolar I
disorder and bipolar II disorder. The lifetime prevalence of MDD Is around
12.2% to 16.2% [2,3] while as the prevalence of bipolar disorder are
significantly lower, ranging from 0.9% to 4.4% [4,5]. In Bipolar disorder I
prevalence has been found to range from 0.8% to 3.3% [6,7] while as in Bipolar
disorder II prevalence has been estimated at around 0.5% to 1.1% [8] The
presence of more than one disorder in a person, for a defined period of time is
referred as Comorbidity[9] Comorbidity can be of three main types:[10]
1. Comorbidity of physical and
psychiatric disorders, e.g. depression and hyperthyroidism;
2. Comorbidity of related disorders, e.g.
anxiety and depression; and
3. Comorbidityof disorders indirectly
related, e.g. psychotic depression and substance abuse.
Comorbid psychiatric disorders usually
precede the onset of bipolar disorder. Bipolar disorder often coexists with
other Axis I and Axis II disordersand studies have found that psychiatric
comorbidity in bipolar disorder range from 50% to 70% [11], In a Study with
bipolar disorder, 65% patients met DSM-IV criteria for at least 1 comorbid
lifetime Axis I disorder, whereas 42% had 2 or more Axis I comorbidities, and
24% had 3 or more [12]. Bipolar patients with psychiatric comorbidity had more
mixed features, depressive episodes, and suicide attempts; poorer outcome and
treatment compliance [10]. In another study, substance use disorders also
follow the onset of bipolar disorder [13]. Sixty percent of premature deaths in
those with serious mental illness are as a result of general medical conditions
[14]. Studies have shown that patients with mood disorders have more comorbid
medical illnesses. Researchhas suggested that that there may be underlying
biological mechanisms linking mood disorder and many medical illnesses [15-18].
The current study will determine the
psychiatric and medical disorders in a sample of patients with bipolar
affective disorder in a general hospital setting.
Aims and Objectives
a) To study the socio-demographic profile
of patients with Bipolar affective disorder.
b) To study the prevalence of psychiatric
comorbidities in patients with Bipolar affective disorder.
c) To study the prevalence of medical
comorbidities in patients with Bipolar affective disorder.
Material and Methods
This cross-sectionalstudy was conducted
at the department of Psychiatry, Sher-I-Kashmir Institute of Medical
Sciences(SKIMS),Medical College and hospital, Bemina, Srinagar, Jammu and
Kashmir. Psychiatry department at SKIMS-MC is a General Hospital Psychiatry
unit. The study was approved by institutional ethical committee.
The patients attending the hospital
outpatient department giving a voluntary consent were included in the study.
The present study was conducted on patients with bipolar affective disorder.
The sample comprised 100 patients attending psychiatry OPD diagnosed as Bipolar
Affective Disorder using ICD 10 during the period of june 2017 to june 2018
[19]. The diagnosis for the study group was confirmed by M.I.N.I (Mini
International Neuropsychiatric Interview) [20]. The following inclusion and
exclusion criteria were used in the study.
Inclusion Criteria for patient:
a) Patients should fulfill ICD -10
criteria for Bipolar affective disorder.
b) Age of the patient should be 18 years
or above.
c) Illness duration of at least 12
months.
d) Patients who are able to provide
informed consent.
Exclusion Criteria for patient:
a) Patients aging below 18 years of age.
b) Patients who are not willing to
participate.
c) Patients who had medical or
psychiatric illness before the diagnosis of BPAD.
Methodology
Instruments:
a) Demographic profile and clinical data
sheet of patients. Intake data of each patient was recorded on a specially
designed proforma. This consisted of details about age, sex, marital status,
educational status, occupation, socioeconomic status, residence, type of
family.
b) International Classification of Mental
and Behavioral Disorders (ICD-10)
[19] Based on the clinical assessment,
the diagnosis was made according to ICD-10 clinical descriptions and diagnostic
guidelines.
c) Mini-International Neuropsychiatric
Interview (M.I.N.I) [20]
The Mini-International Neuropsychiatric
Interview (M.I.N.I.) is a short structured diagnostic interview, developed
jointly by psychiatrists and clinicians in the United States and Europe, for
DSM-IV and ICD-10 psychiatric disorders.
Results
In the present study the mean age of
patients was 34.3 years, Majority of patients i.e. 31% (n=31) were from 30-39
years of age group followed by 26% (n=26) of patients in the age group of 20-29
years ,17% (n=17) in ≥ 50 years,14% (n=14) in the age group of 40-49years and
12% (n=12) < 20years. Majority of BPAD patients were females i.e. 53% (n=53)
and males were 47% (n= 47). Among 100 patients most of them were married 63%
(n=63) and 37% (n= 37) were unmarried with no formal education i.e. 36% (n=36)
, 32% (n=32%) had secondary education, 26% (n=26) were graduate and 6% (n=6)
had primary education. Majority of the patient in our study belonged to low
socioeconomic status i.e.60% (n= 60) and 40% (n=40) belonged to middle
socioeconomic status. Most of patients i.e. 86% (n=86) had rural residence and
14% (n=14) had urban residence (Tables 1-5) and (Figure 1).
In 82% (n=82) of patients there was no
family history of psychiatric illness and in 18% (n=18) of patients, mental
illness in any other family member was present. In present study, 87% (n=87) of
patients, no medical illness was present in family member and 13% (n=13) of
patients had medical illness present in family In this study, obesity/ weight
gain (n=52), chronic headache (n=45), hypertension (n=30), elevated serum
lipids (n=28), thyroid disorders (n=19), diabetes (n=12), GERD (n=9), CAD
(n=4), epilepsy (n=2), COPD (n=2), bronchial Asthma (n=1), Parkinson’s disease
(n=1), CKD (n=1) were among the medical comorbidities. In this study the most
prevalent psychiatric disorders in patients with BPAD were Substance use
disorder (n=32), somatoform disorders (n=18), Generalized anxiety disorder
(n=12), obsessive and compulsive disorder (n=11), panic disorder (n=9), simple
phobia (n=7), eating disorders (n=5), social phobia (n=4), and PTSD (n=2).
Discussion
This study examined the Medical and
psychiatric comorbidity in patients with Bipolar Disorder. Bipolar disorder
(BPD) is highly prevalent disorder by the presence of comorbid conditions and
these comorbidities has negative prognostic implications for psychological and
medical well-being and longevity.[16,17] Bipolar disorders are associated with
psychiatric and medical comorbidities and simultaneous diagnosis and their
treatment is equally important [21,22]. Most patients suffering from bipolar
disorder met criteria for 3 or more lifetime psychiatric disorders. Patients
with bipolar disorder has impairment even during the period of remission due to
physical and psychiatric comorbidities and can lead to disability. WHO
classification of disability have placed BPD seventh in the disability cause
[23-26], The complex mechanisms underlying the comorbidity in Bipolar disorders
may suggest that the causal relationships are likely to be bidirectional
[27,28].
In our sample the medical conditions
associated with bipolar disorder were Obesity/weight gain(52%), Headache (45%),
Hypertension (30%), Elevated serum lipids (28%), Thyroid disorders (19%),
Diabetes (12%), GERD (9%), Coronary artery disease (4%), Epilepsy and COPD 2%
each, Parkinson’s disease, Bronchial Asthma, and chronic kidney disease 1 %
each.
Burden of overweight has increased
rapidly over the past decades globally. Obesity/Overweight are emerging as an
important public health problem in India [29,30]. In India reported prevalence
of overweight in range of 1.5%–24.0%in general population and showed rapid
increase [31]. In our study the 53% patients showed weight gain which is higher
than the prevalence in general population, Patients with Bipolar disorder tend
to be overweight and reason could be the treatment of bipolar disorder
especially valproate, carbamazepine, Lithium and antipsychotics which may also
increase the risk of other comorbid medical disease [32-36].
Another reason for could be the comorbid
eating disorder which includes the excessive carbohydrate consumption and low
rates of exercise [37,38]. Headache is prevalent in every country affecting
both genders and all socioeconomic levels. In general the percentages of the
adult population with an active headache is 46% [41,42].
In our study 47% patients were suffering
from headaches which is almost similar to the prevalence of general population.
The connection between migraines and bipolar disorder is so strong that over
one-third of people living with bipolar suffer from migraines [43,44].
Researchers think that there may be a genetic abnormality in serotonin,
dopamine and glutamine neurotransmitters that contributes to both migraine
headaches and bipolar disorder [45]. Hypertension is an important public health
problem in developed and developing nations [46,47].The prevalence of hypertension
in general population is 20.9% and in our study 30% patients with BPAD was
suffering from hypertension which is higher than the general population [48].
The link between bipolar affective disorder and hypertension depends upon
various factors such as Life styles, obesity and psychotropic medicines in
particular second-generation antipsychotics are likely to play a role [49-51].
The effect of psychotropic medications
and associated weight gain or the complications of treatment with some atypical
antipsychotics may lead to diabetes as well as a marked increase of serum
lipids [52]. A bipolar disorder and metabolic disorders, such as coronary
artery disease and diabetes type 2, have strong genetic links and may share
some common pathophysiological pathways [53]. The comorbidity of thyroid
disorder in individuals with bipolar disorders has a well-established link.
Lithium a mood stabilizer which is a common treatment for bipolar disorder can
also lead to thyroid disorders as a common side-effect of the drug [54]. A
higher burden of medical illness is indicative of a more severe illness course,
with greater impairment in functioning which has been also seen in previously
reported findings.The presence of a medical condition increases the risk of
developing a mood episode/ disorder and vice versa [49]. Bipolar disorder often
coexists with other Axis I disorders.In our study the psychiatric disorders
associated with bipolar affective disorders were Substance use disorder (32%),
somatoform disorders (18%), Generalized anxiety disorder (12%), obsessive and
compulsive disorder (11%), panic disorder (9%), simple phobia (7%8), eating
disorders (5%), social phobia (4%), and PTSD (2%).
Psychiatric disorders with bipolar
disorder compared to their rates in the general population are higher and can
pose a therapeutic challenge as well as a diagnostic dilemma [55]. A careful
assessment, accurate history form bipolar patient is a challenge due to overlap
between symptoms of BPAD and other psychiatric conditions.
Comorbid Substance use disorder was found
to exist in 48- 61% of patients with bipolar affective disorder in some studies
[56-58]. The significant indicator for the course of bipolar disorderisdrug
abusewith regard to the individual and in relation to family history of drug
abuse. Patients with bipolar affective disorder are at higher risk for anxiety
disorders including generalized anxiety disorder, simple phobia, social phobia,
obsessive-compulsive disorder, posttraumatic stress disorder, and panic
disorder [59,60]. Substance use and anxiety disorders are higher in patients
with bipolar disorder than in general population, similar results were found in
our study [61,62].
Conclusion
The current study suggested that patient
suffering from bipolar affective disorder are at increased risk of developing
medical or psychiatric comorbidities. It is very important for the treating
physician to be aware of the prevalent medical and psychiatric conditions
patients with bipolar affective disorders and knowledge of these comorbidities
help in prevention, early detection and treatment of such illnesses as well
will improve treatment response and prognosis in bipolar patients
itself.Awareness among healthcare professionals about the risks to which
patients withaffective disorders are exposed is of great importance, as the
medical illnessesare likely to coexist with a mood disorder, which may help to
improvediagnostics and management and therefore clinical and social carefor
patients. Overall, the presence of comorbidities in BPD has negative prognostic
implications for psychological health and for medical well-being and longevity.
In order to improve quality of life, prognosis and life expectancy for those
with these illnesses, it is important that further researches on this topic
should be continued.
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Psychology And Behavioral Sciences articles Please Click
To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
Monday, 25 November 2019
Lupine Publishers: Lupine Publishers | The Benefits of Sports Medicin...
Lupine Publishers: Lupine Publishers | The Benefits of Sports Medicin...: Lupine Publishers | Journal of Orthopaedics Opinion Physiotherapy and Sports Medicine in a new concept focused not only on...
Friday, 22 November 2019
Lupine Publishers: Lupine Publishers | Utilization of Forecasting Glo...
Lupine Publishers: Lupine Publishers | Utilization of Forecasting Glo...: Lupine Publishers | Journal of Textile and Fashion Designing Editorial Considering the importance of technology and the hu...
Thursday, 21 November 2019
Lupine Publishers: Lupine Publishers | Is the salvation of life on th...
Lupine Publishers: Lupine Publishers | Is the salvation of life on th...: Lupine Publishers- Environmental and Soil Science Journal Before the advent of modern industry, nature had tangible additions in...
Wednesday, 20 November 2019
Lupine Publishers: Lupine Publishers | Evaluation of Host Associated ...
Lupine Publishers: Lupine Publishers | Evaluation of Host Associated ...: Lupine Publishers- Environmental and Soil Science Journal Abstract The water quality of many waterways in the state of ...
Tuesday, 19 November 2019
Lupine Publishers: Lupine Publishers | Crack and Leakage Detection on...
Lupine Publishers: Lupine Publishers | Crack and Leakage Detection on...: Lupine Publishers- Environmental and Soil Science Journal Abstract In this study, a method of water leakage detection s...
Lupine Publishers | Breast Cancer awareness, knowledge and beliefs among Libyan women
Lupine Publishers | Scholarly Journal Of Psychology And Behavioral Sciences





https://lupinepublishers.com/psychology-behavioral-science-journal/fulltext/breast-cancer-awareness-knowledge-and-beliefs-among-libyan-women.ID.000135.php
Abstract
Background: Breast cancer
(BC) is the most frequent cancer of women. The high mortality in developing
countries is associated with late detection, and lack of knowledge among women
and adequate screening programmes.
Objectives: The objectives of
this study are assess the current level and determinants of knowledge and
beliefs regarding (BC), risk factors and various screening methods among Libyan
women.
Methods: A cross-sectional
descriptive study carried out between September and October 2016 among a sample
of adult women in western Libya. Participants were asked to fill a validated
questionnaire to investigate their knowledge about the risk factors as well as
their awareness and screening behaviours of (BC). Data were collected from 1091
woman.
Results: The results of
the study showed the majority of women participated in the study were aware of
BC early warning signs and symptoms with over 90% of the women were able to
list at least one symptom of breast cancer correctly. The most frequent warning
sign identified was breast lump (91.0 %), followed by discharge from the
nipples (80.6%). Also, 565 (52.7%) of those surveyed were aware that increasing
age was associated with a higher incidence of breast cancer and 747 (68.3%) of
the respondents identified positive family history as a risk factor for breast
cancer. Moreover, 62% of female participants know how to perform SBE, and only
59% ever performed BSE. The majority of women in the study (92%) would seek
medical advice if they discovered a mass in the breast whereas, about half of
those (59%) would consult a male doctor.
Conclusions: Women
participated in this study were fairly informed about BC risks and warning
signs; the results appear to reflect growing awareness of women regarding BC
screening methods. health education message should be presented and delivered
in a culturally-sensitive manner and tailored to provide simple and clear
information and avoid false beliefs and misconceptions about the disease, its
screening methods and management options.
Keywords: Breast cancer; Breast cancer
self-examination; awareness; Libya
Introduction
Breast cancer is the most common cancer
in women both in the developed and less developed world. It is estimated that
worldwide over 508 000 women died in 2011 due to breast cancer. Although breast
cancer is thought to be a disease of the developed world, almost 50% of breast
cancer cases and 58% of deaths occur in less developed countries [1]. Breast
cancer (BC) represents 10% of all cancers diagnosed annually and the second principal
cause of cancer deaths in women worldwide [2,3]. The incidence of new cases is
expected to rise from 10 million in 2002-15 million by 2025, with 60% of those
cases occurring in developing countries. Data from the Arab world have placed
breast cancer at the number one position with almost half of cases occurs in
women under the age of 50 [4]. In Libya, breast cancer is accounting for more
than 25% of all cancer in females with age-standardised mortality rate of 10.9
per 100,000 [5]. Breast cancer survival rates vary greatly worldwide, ranging
from 80% or over in North America, Sweden, Japan and Australia to around 60% in
Brazil and Slovakia and below 40% in Algeria [6].
The low survival rates in less developed
countries can be explained mainly by the lack of early detection programmes,
resulting in a high proportion of women presenting with late-stage disease, as
well as by the lack of adequate diagnosis and treatment facilities [1]. WHO
promotes breast cancer control within the context of comprehensive national
cancer control programmes that are integrated to non-communicable diseases and
other related problems. Comprehensive cancer control involves prevention, early
detection, diagnosis and treatment, rehabilitation and palliative care. Raising
general public awareness on the breast cancer problem and the mechanisms to
control as well as advocating for appropriate policies and programmes are key
strategies of population-based breast cancer control [1].
Screening and early detection is widely
recognized as being a principal factor in reducing the mortality from breast
cancer [7]. However, previous studies reported that most breast cancer patients
present at advanced stages of the disease which emphasise the need for
increasing awareness and improved screening programmes including
self-examination, clinical breast examination and mammography [8,9]. In 2011, a
comparison of the clinic-pathological and epidemiological features of breast
cancer in Libya to corresponding data from patients from Nigeria and Finland
has reported that approximately 51% of Libyan patients were classified in
stages 3 and 4 [10,11]. Also, research has shown poor levels of knowledge
towards risk factors awareness and screening methods even among young and
educated women [12-18].
Knowledge deficiency may lead to delayed
presentation with advanced stages when little or no benefit is derived from any
form of therapy. For presentation at an early stage, women must be “breast
aware”; they must be capable of identifying symptoms of BC through routine
practice of screening [19]. Assessment of the current level of breast cancer
awareness and knowledge toward risk factors and screening methods is crucial
for the development of awareness campaigns and programmes for women to decrease
the burden of the disease and mortality. Therefore, the study will be conducted
to assess the current level and determinants of knowledge and beliefs regarding
breast cancer, risk factors and various screening methods among Libyan women.
Materials and Methods
A cross-sectional descriptive study
carried out between September and October 2016 among a sample of adult women in
western Libya. Women participating in the study were interviewed using
pre-tested validated questionnaire. The questionnaire included 49 questions
pertaining three sections:
I. socio demographic characteristics of
women participating in the study;
.
II. knowledge of breast cancer risk
factors and warning signs;
III. Knowledge and awareness of women
towards breast cancer screening methods knowledge (BSE, CBE, and mammography).
Knowledge Scoring
The questionnaire consisted of 23 items
that assessed students’ knowledge related to breast cancer (13 questions related
to BC risk factors and 10 questions related to BC warning signs0 and 20 items
that assessed students’ knowledge regarding breast cancer screening methods.
These questions were then scored; each correct response was scored one (1)
point and each wrong or “don’t know” was scored zero (0). A correct response
was based on literature and current practice. The knowledge index was
calculated for each participant by summing the number of correct answers. The
total score of the participants’ knowledge regarding breast cancer is 23
(100%). The knowledge level was categorised as “low” for scores within 0-49%,
“moderate” for scores within 50-79% and “high” for scores within 80-100% [20].
These scores were then used to assess the relationship between socio-demographic
factors and level of breast cancer knowledge and warning signs.
Statistical Analysis
Data were translated to English and
analysed using SPSS version 17 (SPSS Inc., Chicago, IL). Descriptive statistics
including means, standard deviation, frequencies, and percentages were obtained
for all continues and categorical variables as appropriate. Chi-square test was
used to examine the association between the respondents’ socio-demographic
variables and knowledge of breast cancer.
Ethical Considerations: Permissions were
obtained from the local health directorate and prior orientation of
participants was carried out. The data collection tools were anonymous, and
data confidentiality was maintained throughout the study.
Results
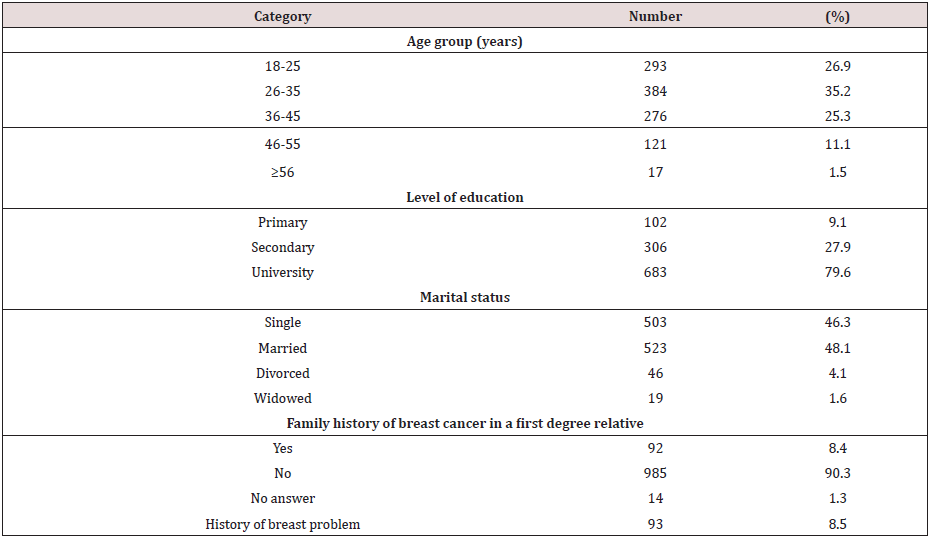
The mean age of the 1091 women enrolled
in the study was 33.2 (SD 9.6; age range: 18-61) years. Most participants
(71.8%) were aged less than 40 years and there were 501 (45.8%) single
respondents; 463 (42.2) were students; 996 (79.6%) had a university degree and
930 (93.4%) had no family history of breast cancer (Table 1).
Table 1: Socio-demographic Characteristics of the
Participants.
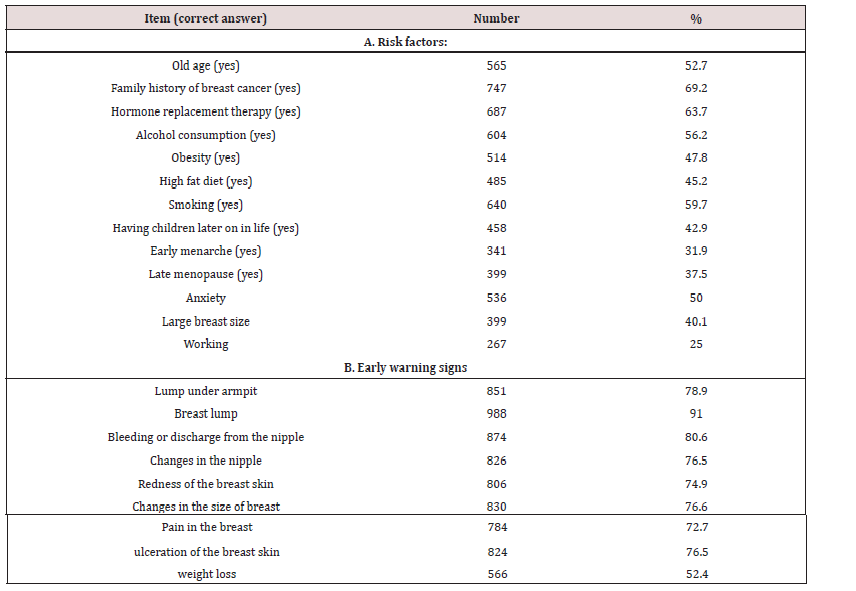
Section A of Table 2 shows respondents’
knowledge of risk factors for breast cancer; The women surveyed had a fair
knowledge of BC risk factors; 565 (52.7%) of those surveyed were aware that
increasing age was associated with a higher incidence of breast cancer and 747
(68.3%) of the respondents identified positive family history as a risk factor
for breast cancer. However, only third of the participants answered correctly
about the effect of early menarche (31.9%) and late menopause (37.5%). The
majority of women participated in the study were aware of BC early warning
signs and symptoms with over 90% of the women were able to list at least one
symptom of breast cancer correctly. The most frequent warning sign identified
was breast lump (91.0 %), followed by discharge from the nipples (80.6%). Only
566 people (52.4%) acknowledged that weight loss could be a warning sign of
breast cancer (Table 2).
Table 2: knowledge regarding Breast cancer risk factors
and warning signs among study participants.
The results showed that 62% of female
participants know how to perform SBE, and only 59%% ever performed BSE. The
majority of women in the study (92%) would seek medical advice if they
discovered a mass in the breast, whereas, about half of those (59%) would
consult a male doctor. Regarding screening methods, women were more familiar
with BSE. Only 20% of participants were not aware of BSE, compared to 40% of
women who were not aware of ultrasound as a BC screening method. In total,
women who didn’t know any screening methods constituted only 4%. While, 45% of
women were familiar with the five screening methods [20].
Figure 1: Distribution of breast cancer risk factors and
warning signs knowledge scores.

Table 3: Relationship between knowledge scores and
demographic variables of the respondents.

Figure 1 shows the distribution of the
knowledge scores amongst the respondents. The median score was 15 with 782
(71.5%) of women scoring >50% and 240 (22%) had a good score of o 80% or
more. Age of the participants, marital status and their level of education did
play a significant role in determining the knowledge attitude, while positive
family history of breast cancer in a first degree relative as well as a history
of breast problem were not significantly associated with BC knowledge (Table
3). Almost 50% of those with good knowledge score aged between 26-35 years and
75% had a university degree. Whereas only 8% of participants with good
knowledge score had a positive family history breast cancer or a previous
breast problem.
Discussion
Breast cancer is the most common of all
female cancers in Libya [5]. In this study, the knowledge and practice among
general population in western Libya was explored. The main findings were that
level of awareness of risk factors and early warning signs of BC was moderate,
with 71.5 % having good knowledge, also the study showed that 59.2% of women
participated in the study perform BSE. The level of knowledge about breast
cancer and the screening behaviour is generally poor in Arabic region compared
to the developed world [6,10,17]. In the present study, respondents answered
correctly that the commonest symptom of breast cancer is a breast mass. Our
results are consistent with those of similar studies carried in Saudi Arabia
[21,22] and Kuwait [23].
The present study showed that women
demonstrated higher knowledge of breast cancer screening and risk factors and
were more likely to perform BSE compared to other recent studies in
neighbouring countries [24-26]. Similar to previous studies [23,25,27] the most
familiar methods was BSE followed by CBE and mammography. As it was expected,
satisfactory knowledge scores were more common among younger participants and
those with higher educational levels. However, unlike other studies in the
region [24-25] and worldwide [28], the anticipated fact that women who had a
breast problem or positive family history of BC would have better knowledge
scores could not be demonstrated in the present study. The study revealed that
about two thirds of the participants shared a misconception that early menarche
and late menopause were not risk factors for BC. This finding was supported by
a previous study [29].
The results of this study may be
influenced by the young age and the relatively high educational level of the
surveyed women which may reflect selection bias. A second limitation of the
current study is the use of convenience sampling to recruit participants which
may limit the generalisability of the findings. Nevertheless, convenience
sampling considered a valid data collection method and has been widely used in
health education research [30]. In spite of these limitations, the study
yielded significant findings that could have implications reorganise the
national health education strategy.
Conclusion
women participated in this study
were fairly informed about BC risks and warning signs; the results appear to
reflect growing awareness of women regarding BC screening methods. However,
health education message should be presented and delivered in a
culturally-sensitive manner and tailored to provide simple and clear
information and avoid false beliefs and misconceptions about the disease, its screening
methods and management options.
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Psychology And Behavioral Science articles Please Click
To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
Monday, 18 November 2019
Lupine Publishers: Lupine Publishers| Waste to Worth - Sludge Contain...
Lupine Publishers: Lupine Publishers| Waste to Worth - Sludge Contain...: Lupine Publishers- Trends in Civil Engineering and its Architecture Opinion Human activities on earth produce in considerabl...
Friday, 15 November 2019
Lupine Publishers: Lupine Publishers| Waste to Worth - Sludge Contain...
Lupine Publishers: Lupine Publishers| Waste to Worth - Sludge Contain...: Lupine Publishers- Trends in Civil Engineering and its Architecture Opinion Human activities on earth produce in considerabl...
Thursday, 14 November 2019
Lupine Publishers: Lupine Publishers | Domestic Violence Perpetration...
Lupine Publishers: Lupine Publishers | Domestic Violence Perpetration...: Lupine Publishers | Journal of Orthopedics Abstract A face is an index of mind correlation, co-efficient of mind. Domesti...
Wednesday, 13 November 2019
Lupine Publishers: Lupine Publishers | Fibre Reinforced Composites: M...
Lupine Publishers: Lupine Publishers | Fibre Reinforced Composites: M...: Lupine Publishers | Journal of Textile and Fashion Designing Introduction Today, at the age of developing newer materials, i...
Tuesday, 12 November 2019
Lupine Publishers | Psychology And Behavioral Sciences
Lupine Publishers | Psycho-Biological Factors of the Formation of Killer Teenagers and Their Prevention

Abstract
The psychobiological factors of the
formation of killer teenagers have been investigated. It was established that
the neurobiological correlate of aggressive killer organisms is serotonin. Its
content in the brain of killer organisms is about 50% lower compared to normal
ones. Psychobiological factors of the prevention of killer organisms’
formation, comprising adequate nutrition and physical exercises have been
demonstrated.
Keywords: Killer Organisms; Serotonin;
Triptophan
Introduction
During last period confrontation between
14-16 years old teenagers resulting in murder, became very frequent. There may
be given many examples of tragedies which happened in different countries, when
young people have died of multiple wounds. Parents, teachers, representatives
of police, school supervisors, psychologists hold active debates by TV-shows
and radio transmissions about the necessity to increase vigilance and activity,
to conduct additional trainings for supervisors; but nobody asks what is the
reason for such cruel behavior among the youth. Several psycho-emotional
factors, responsible for the formation of aggressive and killer organisms have
been distinguished during our multiyear neurochemical studies [1,2]. These are:
1. the aggressive social surrounding in the family; 2. wrong diet; 3. increased
level of sex-hormones (testosterone) in 14-16 years old boy-teenagers; 4.
existence of “war” and “murder” genes, caused by chromosomal disorders; and 5.
TV transmissions, demonstrating and favoring killing, speculating for the
emphatic appreciation of the information by young people.
Since the Italian neurobiologist Giacomo
Rizzolatti has discovered mirror neurons in brain, responsible for perception
of speech and behavior of surrounding people by a newborn, it becomes clear
that if the post natal development of a newborn takes place in an aggressive
social surrounding (fight between family members, violence, usage of narcotics,
alcohol), the aggressive behavior will be encoded in his genetic apparatus.
This information stays in the organism of a person during the whole life and
may be revealed in the form of aggressive behavior of a young person [1,2].
Incomplete nutrition is the second factor for murder. We have established that
the biogenic amine serotonin is one of the neurobiological correlates for the
formation of aggressive and killer organisms. Its deficiency in young organisms
may become reason for aggressive behavior and killing [3-8]. Experimentally it
was demonstrated that feeding of experimental rats with tryptophanpoor food
during 10-12 days, which is the precursor of serotonin, caused decrease of
serotonin content for 50% in experimental animals. As a result these organisms
turned into killers. If the diet was enriched with tryptophan (100mg), rat-killers
turned into peaceful ones, tolerant to frogs and mice. Diversely from normal
rats not a single case of murder was mentioned during contact with them. It
must be taken into account that in aggressive to animals children content of
serotonin, as a rule, is essentially low, as well as in those monkeys, who have
lost the leader’s function in their group. Accordingly, the behavior of
prestige-lost children must be observed attentively at school [4,5].
For the prevention purposes supplying
school buffets with cheeseburgers, prepared of tryptophan-rich Dutch and melted
cheese, which is the precursor of serotonin, is desirable. 100 g of Dutch or
melted cheese contains 790 and 500 g of tryptophan respectively. This amount of
the substance is able to raise thecontent of serotonin in a young organism and
essentially decrease his aggressive behavior. It is well known that isolation
from the society is one additional powerful factor for the formation of an
aggressive person. That’s why the single-child families must take care for
social formation of a child with friends in kinder-gardens, to prevent
aggression [6].
14-16 years is the crucial age for
teenagers and serious changes are mentioned in male hormonal balance at this
period. Special experiments were conducted on animals to reveal the
relationship between aggression and murder and changes of masculine
sexhormones. The experimental rats were castrated. As a result no cases of
aggression or killing have been revealed from castrated animals towards mice
and frogs. While injection of test animals with testosterone changed the
situation in the opposite directioncases of mice and frogs killing by rats
became evident. For the prevention the facts of killing the fatigue tests using
swimming has been done with experimental rats. The result was interesting:
killer rats became again tolerant toward mice and frogs and no case of
aggression or murder has been revealed [6,8,9].
Accordingly, our recommendation to school
supervisors is to increase the physical activity between-lessons of teenagers
for diminishing the content of biologically active compounds in blood, among
them of sex-hormones. We hope that the government will try all the best to
improve the situation to the direction of aggression elimination and healthy
life-style introduction [10,11].
Unfortunately existence of “war” and
“murder” genes in sexchromosomes is reality. According to experimental data
four groups of aggressive and criminal behavior persons are distinguished:
a) young men with Klinfelter syndrome.
They have XXYY set of sex-chromosomes, small testicles, are taller than
average; due to mental deficiency it is easy to involve them in criminal.
b) Young males with aberrant XYY or XXYY
sex-chromosomes. They are tall, with mental deficiency, are distinguished with
aggression and criminal activity.
c) Young men with hereditary disorder of
nervous system. They are distinguished with emotional-ethic degradation,
epileptic anxiety, dogmatism, schizoid personality and alcoholinduced
disorders.
d) 1/4 of the single-egg twins are
inclined to criminal activity. These children must be under the permanent
observation of psychologists for evaluation of their behavior.
All above mentioned indicates that school
psychologist have to know deeply the genetic picture of each school-boy, to
forecast their future behavior and prevent possible criminal prevention
[3,5,6].
Conclusion
Psycho-social factors of murder
formation have been established. It was demonstrated that one of the neural
correlates in killer’s brain is serotonin, which content is by 50% lower in
brains of aggressive killer organisms. The ways of prevention of aggressive
behavior by adequate diet and physical activity is offered
For more Lupine Publishers Open Access Journals Please visit our website: https://lupinepublishersgroup.com/
For more Psychology And Behavioral Sciences articles Please Click
To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
Subscribe to:
Comments (Atom)
-
Abstract Peer pressure is one thing that every individual is vulnerable to and has faced before at some point in their lives. It is beco...
-
 Detaching: Now If the Good Goes by Gabriel Miranda Nava in SJPBS in Lupinepublishers The last time we talked about attachmen...
Detaching: Now If the Good Goes by Gabriel Miranda Nava in SJPBS in Lupinepublishers The last time we talked about attachmen... -
Lupine Publishers | Scholarly Journal of Psychology and Behavioral Sciences Introduction Thomas Hobbes (1588-1679) proposed that voluntary...
